





Abstract
Public health measures targeting coronavirus disease 2019 have potential to impact transmission of other respiratory viruses. We found 98.0% and 99.4% reductions in respiratory syncytial virus and influenza detections, respectively, in Western Australian children through winter 2020 despite schools reopening. Border closures have likely been important in limiting external introductions.
(See the , and the and .)
Coronavirus disease 2019 (COVID-19) has had a profound impact in 2020, with a broad range of public health measures implemented regionally that are targeted at controlling transmission of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Interventions have included physical distancing, stay-at-home orders, school closures, travel restrictions, and border closures. Measures not specific to SARS-CoV-2, therefore, have the potential to impact transmission of other respiratory viruses. The initiation of COVID-19 restrictions in the Northern Hemisphere coincided with the end of winter, with some reports documenting a concurrent early end to local influenza and respiratory syncytial virus (RSV) seasons [1, 2]. In contrast, restrictions in Australia were implemented just prior to the Southern Hemisphere winter, the usual period of peak local RSV and influenza infections [3].
Western Australia (WA) covers the western third of Australia, with a population of 2.64 million, of which the majority are concentrated in a single metropolitan area [4]. WA has experienced minimal local transmission of SARS-CoV-2, with the majority of cases (562 of 655) linked to international travel. Community SARS-CoV-2 transmission has been absent since the end of April 2020 [5], allowing a staged relaxation of lockdown measures while WA state borders to international and interstate travelers have remained closed.
To date, there are limited data that describe the impact of COVID-19 restrictions on influenza and RSV transmission through the Southern Hemisphere winter. In addition, the combination of relaxation of internal COVID-19 restrictions in WA and ongoing border closures represent a unique setting to observe the relative impact of these measures on influenza and RSV activity. Our aim in this study was to describe the weekly detection of pediatric RSV and influenza through winter 2020 in WA compared with the previous 8 seasons in the context of local COVID-19 restrictions.
METHODS
Laboratory data were prospectively collected as part of routine regional public health surveillance, collated per week, from 1 January 2012 to 30 August 2020. Cases were defined as detections of influenza or RSV by validated nucleic acid or antigen detection kits in children (aged <16 years) resident in the metropolitan area. Laboratory results were provided by PathWest Laboratory Medicine, the only public pathology provider to the state that services all but 3 hospitals that admit pediatric patients in WA. Samples were drawn from all public hospitals and emergency departments. Average epidemic curves for the period 2012 to 2019 were calculated using a World Health Organization (WHO) described method [6].
Timeline of Public Health Measures
As part of a national response, the international border was closed to nonresidents on 20 March (week 12). On 6 April (week 15), the WA state border was closed to other Australian states. Borders remain closed at the time of writing. Exemptions are required to enter from interstate locations, and quarantine of all arrivals for 14 days is mandatory [7].
State-wide stay-at-home restrictions were in place from 29 March to 27 April and included a concurrent extended school holiday period (weeks 14–17; Figure 1, period 1). From 27 April restrictions were sequentially lifted; schools were reopened on 29 April with increased cleaning and some physical distancing measures (weeks 18–26; Figure 1, period 2). From 27 June to present (week 27 onward; Figure 1, period 3), while physical distancing and respiratory hygiene continue to be encouraged, the majority of local restrictions were removed, except the limitation of major sport and entertainment venues to 50% capacity. Schools have returned to all normal activities with no limits on size of student gatherings [7].
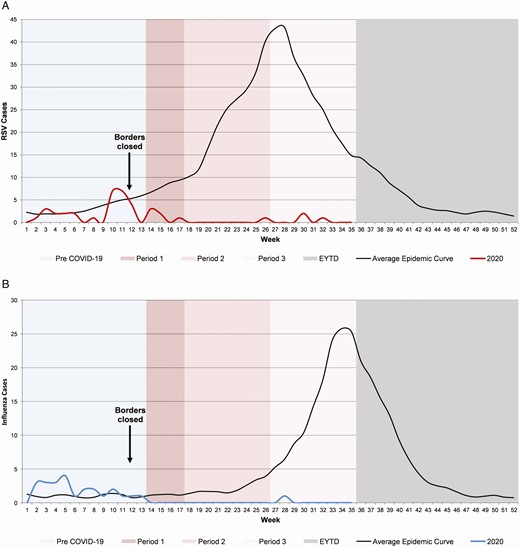
Respiratory syncytial virus (A) and influenza (B) detections in children from metropolitan Western Australian to the end of winter 2020 in the context of COVID-19 restrictions compared with the average epidemic curve (2012–2019). Borders closed: week 12, international borders closed to all nonresidents; 14-day quarantine required for all arrivals. Period 1: week 14 to week 17, state-wide stay-at-home restrictions in place with school holidays extended; borders closed to interstate travelers (week 14). Period 2: week 18 to week 26, restrictions sequentially lifted, allowing gatherings of 10 (week 18), 20 (week 21), and 100 (week 24) people; schools reopened with increased cleaning and some physical distancing measures. Period 3: week 27 to week 35, majority of local restrictions removed, except the limitation of major sport and entertainment venues to 50% capacity; schools returned to all normal activities. Abbreviations: COVID-19, coronavirus disease 2019; EYTD, end of year to date.
RESULTS
During the period 2012–2019, the annual number of RSV cases ranged from 532 to 707 (mean, 629), with the median epidemic peak occurring in week 27. For influenza, annual cases ranged from 134 to 498 (mean, 278), with the median epidemic peak occurring in week 34 (Figure 1).
For the first 13 weeks of 2020, prior to local COVID-19 restrictions, RSV (n = 29) and influenza (n = 24) detections were comparable to the average of previous seasons (Figure 1). Following the initiation of local COVID-19 restrictions in week 14, influenza and RSV activity declined and remained very low relative to previous seasons, even following the sequential relaxation of local COVID-19 restrictions. A total of 10 cases of RSV and 1 case of influenza were detected from week 14 to week 35. Compared with average detections from week 14 to week 35 in prepandemic years, RSV detections were 98.0% lower and influenza detections were 99.4% lower.
The total number of samples tested in 2020 was higher than in previous seasons, thus the percentages of positive tests for RSV (0.28%) and influenza (0.03%) from week 14 to week 35 were substantially lower than in previous seasons (2012–2019 range for RSV, 23.3%–30.4%; for influenza, 3.6%–16.4%).
DISCUSSION
The initial public health measures implemented in WA likely facilitated rapid control of SARS-CoV-2 transmission. The implementation of these measures coincided with the period leading into winter, when RSV and influenza detections peak locally. Early regional reports from Australia indicated an initial decline in respiratory virus detection [8] and related hospital admissions [9] immediately following the implementation of COVID-19 restrictions. We observed a similar initial reduction in RSV and influenza detections among WA children followed by a near complete absence over the subsequent 4 months, confirming that low RSV and influenza activity has been sustained in WA throughout the winter period (weeks 23–35).
Earlier reports from the Northern Hemisphere attributed the observed shortening of influenza and RSV seasons to the implementation of local COVID-19 restrictions [1, 2]. We observed persistent low influenza and RSV activity, even following the relaxation of local COVID-19 restrictions, indicating international and perhaps, to a lesser extent, national border restrictions may have played an important role by preventing external introductions of these viruses. In WA, schools reopened in late April; attendance was >85% by mid-May [10]. School-aged children play a central role in the transmission of both influenza and RSV [11, 12]. At the time of writing, schools have remained open at almost full capacity for 4 months without a notable increase in RSV and influenza detections. Although physical distancing and improved hygiene are likely contributing factors [13], the scarcity of RSV and influenza cases is consistent with the absence of a sizable local reservoir.
It has been hypothesized that changes in health-seeking behavior in the setting of COVID-19 restrictions may have contributed to observed reductions in influenza and RSV activity [9, 14]. Notably, the percentage of positive of tests collected, a frequently used marker for underdetection, remained very low for influenza and RSV throughout the winter period in 2020. Furthermore, a relative return to normal health-seeking behavior would be anticipated in WA in the absence of local SARS-CoV-2 transmission and relaxation of local restrictions. The persistence of low RSV and influenza activity in this setting is likely consistent with a true lack of local infections.
There are wide-ranging potential implications of the observed low RSV and influenza activity. For RSV, with a large cohort of immunologically naive children and low-level local transmission, a delayed peak may yet be observed. Alternatively, the following RSV season may be more extensive than in previous years, with greater morbidity across age ranges. Considering the year-to-year variation in influenza peak and rate of infections, and the absence of clear ongoing transmission currently, it is uncertain whether a delayed local influenza season will occur this year. Similar to RSV, a reduction in population immunity related to current reduced influenza transmission may render the population more vulnerable in the following season. Considering the broader reduction in Southern Hemisphere influenza detections evident in WHO surveillance data [14], together with the likely persistence of some travel restrictions, the Northern Hemisphere may experience a similarly attenuated influenza season in the coming winter. However, protective local COVID-19 restrictions will likely have been lifted in some regions. Conversely, influenza vaccine development may be hampered by a lack of Southern Hemisphere reference samples, limiting the ability to predict potential circulating strains.
A relative strength of this study is its use of data collated as part of existing surveillance activities, which were ongoing prior to the emergence of COVID-19. In addition, the elimination of local SARS-CoV-2 transmission with resultant relaxation of restrictions, including the reopening of schools, is relatively unique to WA. This will facilitates the assessment of the relative impact of initial local restrictions and ongoing border closures on viral detections.
Our analysis does not include hospital admission data. As our surveillance data are drawn from hospitals and emergency departments, we cannot completely exclude that changes in health-seeking behavior related to COVID-19 may have impacted viral detections in 2020. We are planning to assess pediatric emergency department and hospital admission data for overall health service use patterns by diagnosis and age group to examine the broader impact of COVID-19 restrictions.
Following implementation of COVID-19 restrictions just prior to winter, RSV and influenza activity has remained low in WA, even following relaxation of internal restrictions. This is likely due to the impact of external border closures and the resultant prevention of viral introductions. The impact of reduced local RSV and influenza activity on the Northern Hemisphere winter season and future local seasons remains uncertain and warrants ongoing surveillance.
Notes
Financial support. This was an investigator-initiated project supported by a clinician–scientist partnership grant from the Wesfarmers Centre for Vaccines and Infectious Diseases (2020). D. K. Y. is supported by an Australian Government Research Training Program Postgraduate Scholarship. A. O. M. is supported by a National Health and Medical Research Council (NHMRC) Postgraduate Scholarship (1191465) and an Australian Government Research Training Program Fees Offset. A. C. M. is supported by a Raine Clinician Research Fellowship. C. C. B. is supported by an NHMRC Career Development Fellowship (GNT1111596). H. C. M. is supported by a Telethon Kids Institute Emerging Research Leader Fellowship.
Potential conflicts of interest. The authors: No reported conflicts of interest. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest.
References
Author notes
D. K. Y. and D. A. F. contributed equally to this work.


{kind=link}
Comments