Long-Term Coffee Consumption Is Associated with Decreased Incidence of New-Onset Hypertension: A Dose–Response Meta-Analysis

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Selection
2.2. Data Extraction
2.3. Study Quality Assessment
2.4. Statistical Analysis
3. Results
3.1. Study Characteristics
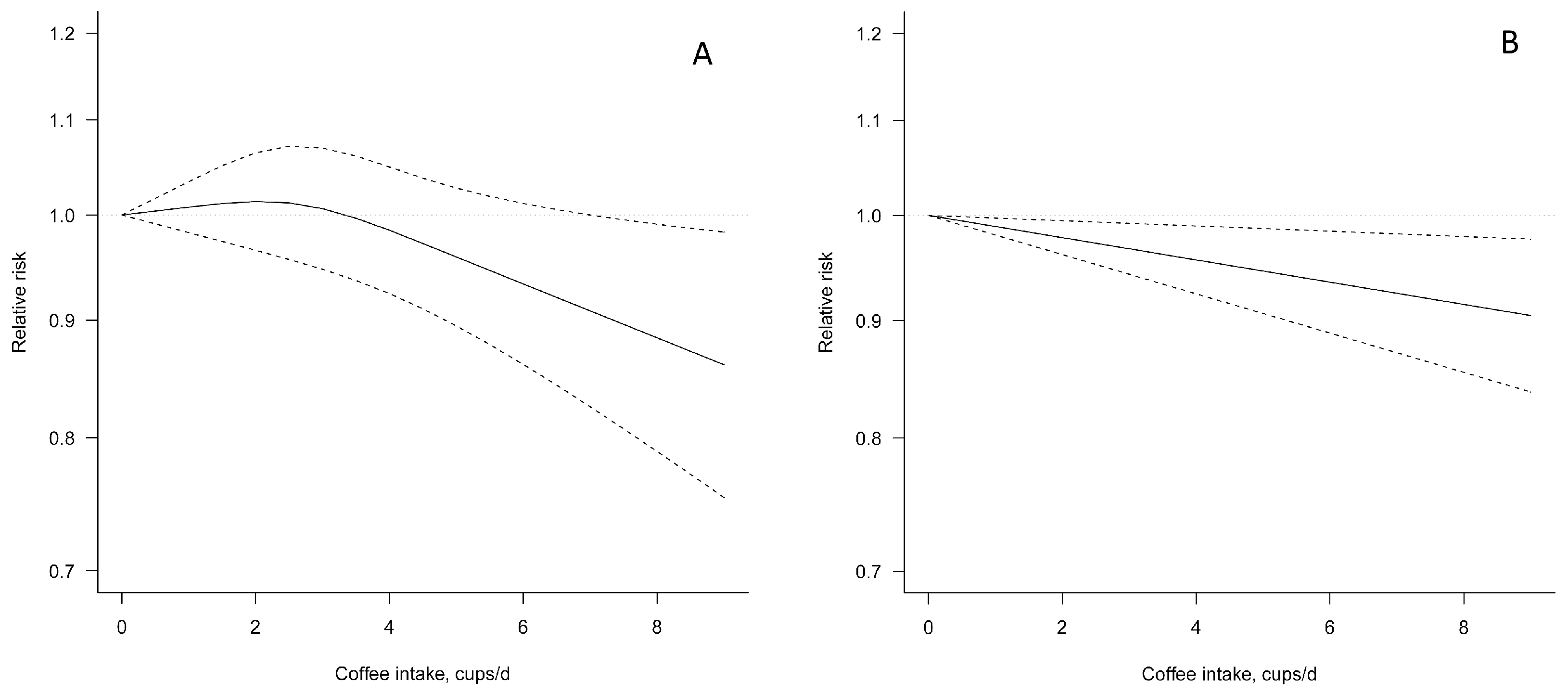
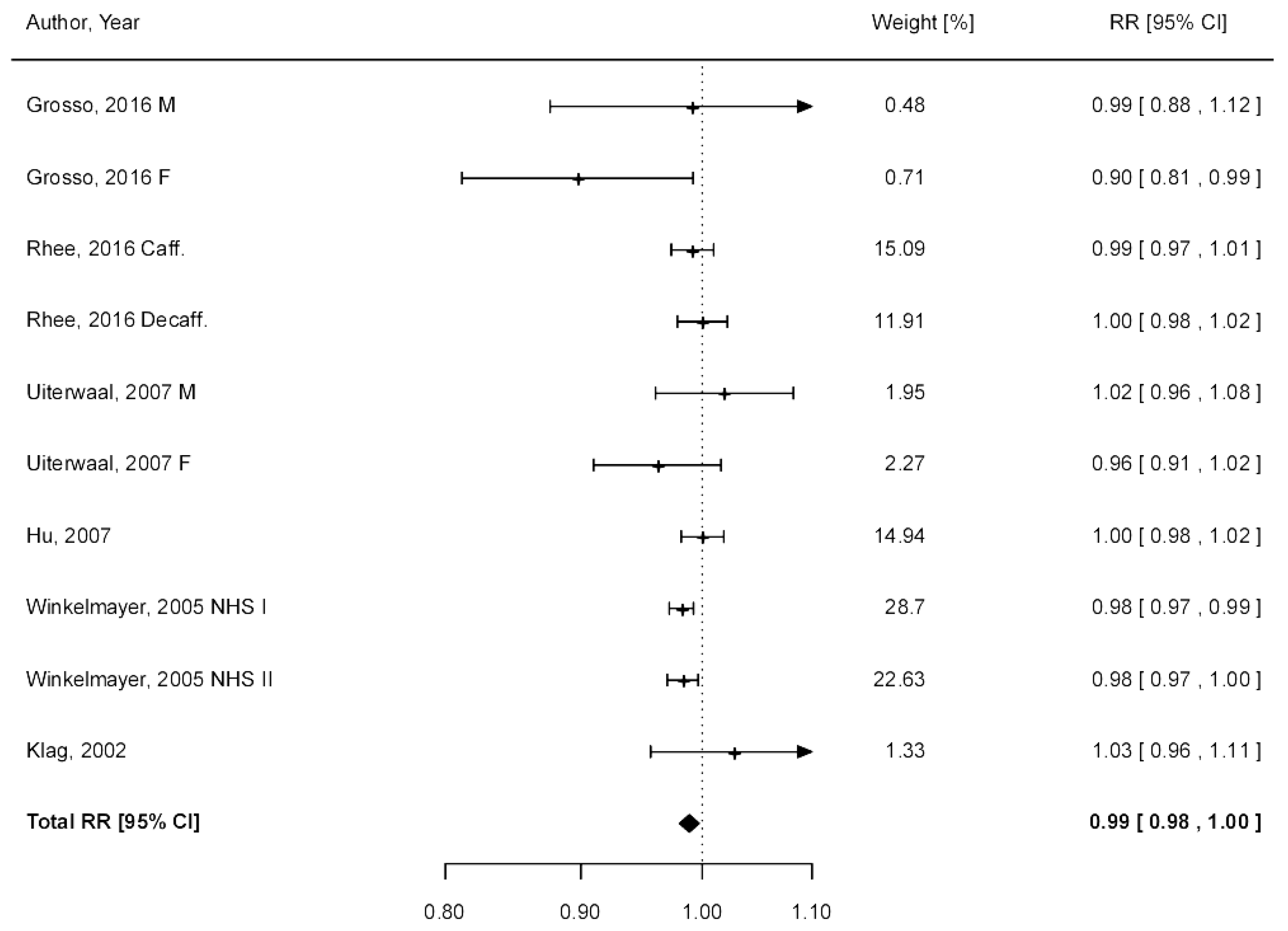
3.2. Coffee Consumption and Risk of Hypertension
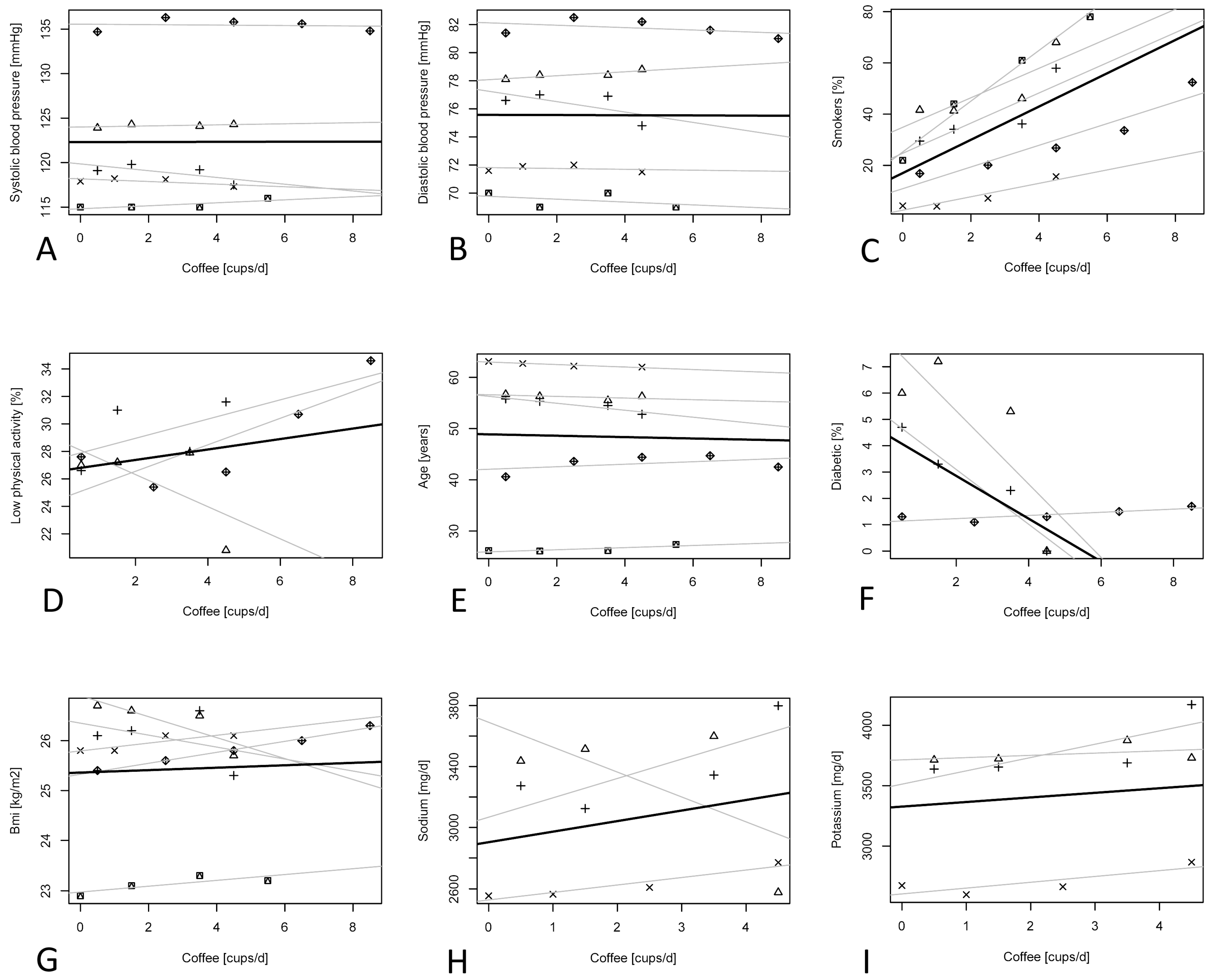
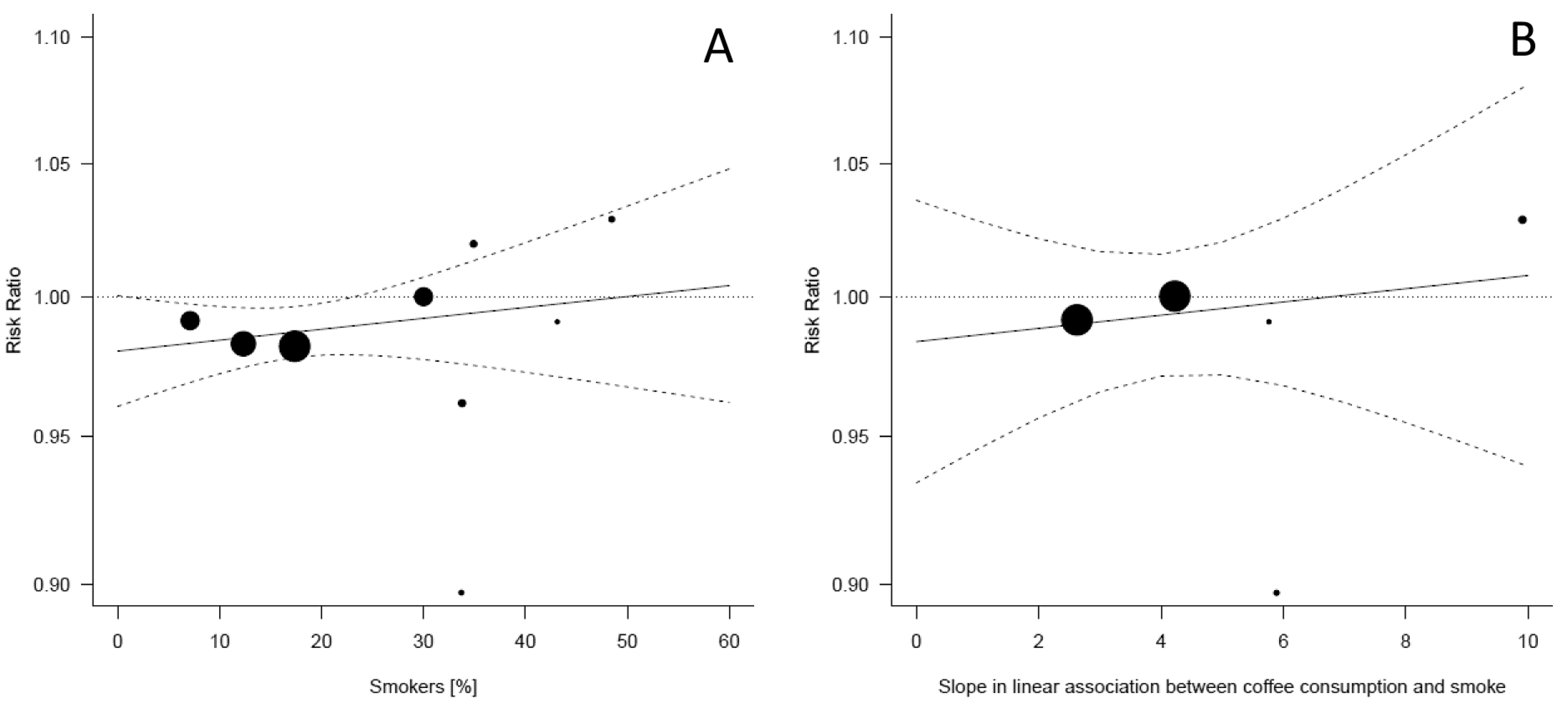
3.3. Potential Confounding Factors
4. Discussion
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Grosso, G.; Godos, J.; Galvano, F.; Giovannucci, E.L. Coffee, Caffeine, and Health Outcomes: An Umbrella Review. Annu. Rev. Nutr. 2017, 37. [Google Scholar] [CrossRef]
- Godos, J.; Pluchinotta, F.R.; Marventano, S.; Buscemi, S.; Li Volti, G.; Galvano, F.; Grosso, G. Coffee components and cardiovascular risk: Beneficial and detrimental effects. Int. J. Food Sci. Nutr. 2014, 65, 925–936. [Google Scholar] [CrossRef] [PubMed]
- Higdon, J.V.; Frei, B. Coffee and health: A review of recent human research. Crit. Rev. Food Sci. Nutr. 2006, 46, 101–123. [Google Scholar] [CrossRef] [PubMed]
- Buscemi, S.; Marventano, S.; Antoci, M.; Cagnetti, A.; Castorina, G.; Galvano, F.; Marranzano, M.; Mistretta, A. Coffee and metabolic impairment: An updated review of epidemiological studies. NFS J. 2016, 3, 1–7. [Google Scholar] [CrossRef]
- Ding, M.; Bhupathiraju, S.N.; Satija, A.; van Dam, R.M.; Hu, F.B. Long-term coffee consumption and risk of cardiovascular disease: A systematic review and a dose-response meta-analysis of prospective cohort studies. Circulation 2014, 129, 643–659. [Google Scholar] [CrossRef] [PubMed]
- Marventano, S.; Salomone, F.; Godos, J.; Pluchinotta, F.; Del Rio, D.; Mistretta, A.; Grosso, G. Coffee and tea consumption in relation with non-alcoholic fatty liver and metabolic syndrome: A systematic review and meta-analysis of observational studies. Clin. Nutr. 2016, 35, 1269–1281. [Google Scholar] [CrossRef] [PubMed]
- Brown, O.I.; Allgar, V.; Wong, K.Y. Coffee reduces the risk of death after acute myocardial infarction: A meta-analysis. Coron. Artery Dis. 2016, 27, 566–572. [Google Scholar] [CrossRef] [PubMed]
- Larsson, S.C.; Drca, N.; Jensen-Urstad, M.; Wolk, A. Coffee consumption is not associated with increased risk of atrial fibrillation: Results from two prospective cohorts and a meta-analysis. BMC Med. 2015, 13, 207. [Google Scholar] [CrossRef] [PubMed]
- Panza, F.; Solfrizzi, V.; Barulli, M.R.; Bonfiglio, C.; Guerra, V.; Osella, A.; Seripa, D.; Sabba, C.; Pilotto, A.; Logroscino, G. Coffee, tea, and caffeine consumption and prevention of late-life cognitive decline and dementia: A systematic review. J. Nutr. Health Aging 2015, 19, 313–328. [Google Scholar] [CrossRef] [PubMed]
- Solfrizzi, V.; Panza, F.; Imbimbo, B.P.; D’Introno, A.; Galluzzo, L.; Gandin, C.; Misciagna, G.; Guerra, V.; Osella, A.; Baldereschi, M.; et al. Coffee consumption habits and the risk of mild cognitive impairment: The italian longitudinal study on aging. J. Alzheimers Dis. 2015, 47, 889–899. [Google Scholar] [CrossRef] [PubMed]
- Noordzij, M.; Uiterwaal, C.S.; Arends, L.R.; Kok, F.J.; Grobbee, D.E.; Geleijnse, J.M. Blood pressure response to chronic intake of coffee and caffeine: A meta-analysis of randomized controlled trials. J. Hypertens. 2005, 23, 921–928. [Google Scholar] [CrossRef] [PubMed]
- Jee, S.H.; He, J.; Whelton, P.K.; Suh, I.; Klag, M.J. The effect of chronic coffee drinking on blood pressure: A meta-analysis of controlled clinical trials. Hypertension 1999, 33, 647–652. [Google Scholar] [CrossRef] [PubMed]
- Steffen, M.; Kuhle, C.; Hensrud, D.; Erwin, P.J.; Murad, M.H. The effect of coffee consumption on blood pressure and the development of hypertension: A systematic review and meta-analysis. J. Hypertens. 2012, 30, 2245–2254. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Hu, G.; Caballero, B.; Appel, L.; Chen, L. Habitual coffee consumption and risk of hypertension: A systematic review and meta-analysis of prospective observational studies. Am. J. Clin. Nutr. 2011, 93, 1212–1219. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses; Ottawa Health Research Institute: Ottawa, ON, Canada, 1999. [Google Scholar]
- Greenland, S. Quantitative methods in the review of epidemiologic literature. Epidemiol. Rev. 1987, 9, 1–30. [Google Scholar] [CrossRef]
- Greenland, S.; Longnecker, M.P. Methods for trend estimation from summarized dose-response data, with applications to meta-analysis. Am. J. Epidemiol. 1992, 135, 1301–1309. [Google Scholar] [CrossRef] [PubMed]
- Orsini, N.; Bellocco, R.; Greenland, S. Generalized least squares for trend estimation of summarized dose-response data. Stata J. 2006, 6, 40–57. [Google Scholar]
- Orsini, N.; Li, R.; Wolk, A.; Khudyakov, P.; Spiegelman, D. Meta-analysis for linear and nonlinear dose-response relations: Examples, an evaluation of approximations, and software. Am. J. Epidemiol. 2012, 175, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Stukel, T.A.; Demidenko, E. Two-stage method of estimation for general linear growth curve models. Biometrics 1997, 53, 720–728. [Google Scholar] [CrossRef] [PubMed]
- Becker, B.J.; Wu, M.-J. The synthesis of regression slopes in meta-analysis. Stat. Sci. 2007, 22, 414–429. [Google Scholar] [CrossRef]
- Klag, M.J.; Wang, N.Y.; Meoni, L.A.; Brancati, F.L.; Cooper, L.A.; Liang, K.Y.; Young, J.H.; Ford, D.E. Coffee intake and risk of hypertension: The johns hopkins precursors study. Arch. Intern. Med. 2002, 162, 657–662. [Google Scholar] [CrossRef] [PubMed]
- Winkelmayer, W.C.; Stampfer, M.J.; Willett, W.C.; Curhan, G.C. Habitual caffeine intake and the risk of hypertension in women. JAMA 2005, 294, 2330–2335. [Google Scholar] [CrossRef] [PubMed]
- Hu, G.; Jousilahti, P.; Nissinen, A.; Bidel, S.; Antikainen, R.; Tuomilehto, J. Coffee consumption and the incidence of antihypertensive drug treatment in finnish men and women. Am. J. Clin. Nutr. 2007, 86, 457–464. [Google Scholar] [PubMed]
- Uiterwaal, C.S.; Verschuren, W.M.; Bueno-de-Mesquita, H.B.; Ocke, M.; Geleijnse, J.M.; Boshuizen, H.C.; Peeters, P.H.; Feskens, E.J.; Grobbee, D.E. Coffee intake and incidence of hypertension. Am. J. Clin. Nutr. 2007, 85, 718–723. [Google Scholar] [PubMed]
- Grosso, G.; Stepaniak, U.; Polak, M.; Micek, A.; Topor-Madry, R.; Stefler, D.; Szafraniec, K.; Pajak, A. Coffee consumption and risk of hypertension in the polish arm of the hapiee cohort study. Eur. J. Clin. Nutr. 2016, 70, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Rhee, J.J.; Qin, F.; Hedlin, H.K.; Chang, T.I.; Bird, C.E.; Zaslavsky, O.; Manson, J.E.; Stefanick, M.L.; Winkelmayer, W.C. Coffee and caffeine consumption and the risk of hypertension in postmenopausal women. Am. J. Clin. Nutr. 2016, 103, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Beltran-Sanchez, H.; Finch, C.E.; Crimmins, E.M. Twentieth century surge of excess adult male mortality. Proc. Natl. Acad. Sci. USA 2015, 112, 8993–8998. [Google Scholar] [CrossRef] [PubMed]
- Yang, A.; Palmer, A.A.; de Wit, H. Genetics of caffeine consumption and responses to caffeine. Psychopharmacology 2010, 211, 245–257. [Google Scholar] [CrossRef] [PubMed]
- Djordjevic, N.; Ghotbi, R.; Jankovic, S.; Aklillu, E. Induction of CYP1A2 by heavy coffee consumption is associated with the CYP1A2 −163C>A polymorphism. Eur. J. Clin. Pharmacol. 2010, 66, 697–703. [Google Scholar] [CrossRef] [PubMed]
- Cornelis, M.C.; El-Sohemy, A.; Kabagambe, E.K.; Campos, H. Coffee, CYP1A2 genotype, and risk of myocardial infarction. JAMA 2006, 295, 1135–1141. [Google Scholar] [CrossRef] [PubMed]
- Palatini, P.; Dorigatti, F.; Santonastaso, M.; Cozzio, S.; Biasion, T.; Garavelli, G.; Pessina, A.C.; Mos, L. Association between coffee consumption and risk of hypertension. Ann. Med. 2007, 39, 545–553. [Google Scholar] [CrossRef] [PubMed]
- Bankir, L.; Perucca, J.; Norsk, P.; Bouby, N.; Damgaard, M. Relationship between sodium intake and water intake: The false and the true. Ann. Nutr. Metab. 2017, 70, 51–61. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Bella, F.; Godos, J.; Sciacca, S.; Del Rio, D.; Ray, S.; Galvano, F.; Giovannucci, E.L. Possible role of diet in cancer: Systematic review and multiple meta-analyses of dietary patterns, lifestyle factors, and cancer risk. Nutr. Rev. 2017, 75, 405–419. [Google Scholar] [CrossRef]
- Zhao, Y.; Wang, J.; Ballevre, O.; Luo, H.; Zhang, W. Antihypertensive effects and mechanisms of chlorogenic acids. Hypertens. Res. 2012, 35, 370–374. [Google Scholar] [CrossRef] [PubMed]
- Sato, Y.; Itagaki, S.; Kurokawa, T.; Ogura, J.; Kobayashi, M.; Hirano, T.; Sugawara, M.; Iseki, K. In vitro and in vivo antioxidant properties of chlorogenic acid and caffeic acid. Int. J. Pharm. 2011, 403, 136–138. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, A.; Yamamoto, M.; Jokura, H.; Fujii, A.; Tokimitsu, I.; Hase, T.; Saito, I. Ferulic acid restores endothelium-dependent vasodilation in aortas of spontaneously hypertensive rats. Am. J. Hypertens. 2007, 20, 508–513. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, A.; Yamamoto, N.; Jokura, H.; Yamamoto, M.; Fujii, A.; Tokimitsu, I.; Saito, I. Chlorogenic acid attenuates hypertension and improves endothelial function in spontaneously hypertensive rats. J. Hypertens. 2006, 24, 1065–1073. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | Name of Cohort (Years of Recruitment), Country | Cohort Size | No. of Cases | Gender | Exposure Variables | Follow-Up Duration | Adjusted Variables |
|---|---|---|---|---|---|---|---|
| Grosso, 2016 (21) | HAPIEE Cohort Study (2002–2008), Poland | 2725 | 1735 | MF | Caffeinated and decaffeinated coffee | 5 y | Age, gender, education, occupation, BMI, alcohol consumption, smoking status, physical activity level, past history of CVD and diabetes at baseline, cholesterol therapy at baseline, total energy intake, vitamin supplement use, oral contraceptive use, and intake of sodium and potassium. |
| Rhee, 2016 (22) | WHI Observational Study, (1993), US | 29,985 | 5566 | F | Caffeinated coffee | 3 y | Age, baseline blood pressure, BMI, physical activity, hormone replacement therapy, alcohol consumption, smoking status, total calorie intake, and intake of sodium, magnesium, calcium, potassium, and phosphorus as time-varying covariates. |
| Uiterwaal, 2007 (20) | DCS (1987–2002), The Netherlands | 6368 | 956 | MF | Caffeinated and decaffeinated coffee | 11 y | Baseline age, sex, height and weight, smoking, alcohol intake, tea intake, education level, occupational status, and total energy intake. |
| Hu, 2007 (19) | Four independent surveys, (1982–2002), Finland | 24,710 | 2505 | MF | Caffeinated and decaffeinated coffee | 13.2 y | Year, education, leisure-time physical activity, smoking status, alcohol consumption, tea consumption, frequency of vegetable, fruit, sausage, and bread consumption, BMI, history of diabetes and total cholesterol, and baseline systolic blood pressure. |
| Winkelmayer, 2005 (18) | NHS I (1976–2002), US | 53,175 | 19,541 | F | Caffeinated coffee | 12 y | Age, BMI, alcohol consumption, family history of hypertension, physical activity, and smoking status, and intake of other beverages. |
| Winkelmayer, 2005 (18) | NHS II (1989–2003), US | 87,369 | 13,536 | F | Caffeinated coffee | 12 y | Age, BMI, alcohol consumption, family history of hypertension, oral contraceptive use, physical activity, and smoking status, and intake of other beverages. |
| Klag, 2002 (17) | JHPS (1947–1995), US | 1017 | 281 | M | Caffeinated coffee | 33 y | Parental history of hypertension, time-dependent number of cigarettes smoked, alcohol intake, physical activity, BMI. |
| No. of Datasets (No. of Studies) | Coffee Intake (Cups/Day) | I2 | Pheterogeneity | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | ||||
| All | |||||||||||
| Non-linear | 10 (6) | Ref. | 1.01 (0.98–1.03) | 1.01 (0.97–1.06) | 1.01 (0.95–1.07) | 0.98 (0.92–1.05) | 0.96 (0.89–1.03) | 0.93 (0.86–1.01) | 0.91 (0.83–1.00) | 51% | 0.004 |
| Linear | 10 (6) | Ref. | 0.99 (0.98–1.00) | 0.98 (0.96–0.99) | 0.97 (0.94–0.99) | 0.96 (0.92–0.99) | 0.95 (0.91–0.99) | 0.94 (0.89–0.98) | 0.92 (0.87–0.98) | 21% | 0.241 |
| Males | |||||||||||
| Non-linear | 3 (3) | Ref. | 1.09 (0.94–1.27) | 1.19 (0.89–1.58) | 1.24 (0.88–1.76) | 1.23 (0.89–1.69) | 1.19 (0.9–1.59) | 1.16 (0.86–1.55) | 1.12 (0.79–1.59) | 0% | 0.458 |
| Linear | 3 (3) | Ref. | 1.02 (0.98–1.06) | 1.04 (0.95–1.13) | 1.06 (0.93–1.21) | 1.08 (0.91–1.28) | 1.1 (0.89–1.36) | 1.12 (0.86–1.45) | 1.14 (0.84–1.55) | 0% | 0.458 |
| Females | |||||||||||
| Non-linear | 4 (4) | Ref. | 1.00 (0.97–1.03) | 1.00 (0.94–1.05) | 0.98 (0.92–1.04) | 0.95 (0.91–0.99) | 0.92 (0.88–0.95) | 0.88 (0.84–0.94) | 0.85 (0.78–0.93) | 43% | 0.059 |
| Linear | 6 (4) | Ref. | 0.99 (0.98–0.99) | 0.97 (0.95–0.99) | 0.96 (0.93–0.98) | 0.94 (0.91–0.98) | 0.93 (0.89–0.97) | 0.92 (0.87–0.97) | 0.90 (0.85–0.96) | 26% | 0.232 |
| Caffeinated coffee | |||||||||||
| Non-linear | 4 (3) | Ref. | 1.00 (0.97–1.02) | 0.99 (0.95–1.04) | 0.98 (0.93–1.03) | 0.95 (0.92–0.99) | 0.92 (0.89–0.96) | 0.9 (0.84–0.96) | 0.87 (0.79–0.96) | 44% | 0.095 |
| Linear | 4 (3) | Ref. | 0.98 (0.98–0.99) | 0.97 (0.95–0.98) | 0.95 (0.93–0.98) | 0.94 (0.91–0.97) | 0.92 (0.89–0.96) | 0.91 (0.87–0.95) | 0.9 (0.85–0.94) | 0% | 0.529 |
| Europe | |||||||||||
| Non-linear | 5 (3) | Ref. | 1.02 (0.9–1.16) | 1.04 (0.81–1.33) | 1.06 (0.76–1.48) | 1.08 (0.8–1.47) | 1.12 (0.92–1.35) | 1.15 (0.98–1.35) | 1.19 (0.91–1.55) | 54% | 0.025 |
| Linear | 5 (3) | Ref. | 0.99 (0.96–1.02) | 0.97 (0.91–1.04) | 0.96 (0.87–1.05) | 0.95 (0.83–1.07) | 0.93 (0.79–1.09) | 0.92 (0.76–1.11) | 0.91 (0.72–1.13) | 38% | 0.166 |
| US | |||||||||||
| Non-linear | 3 (3) | Ref. | 1 (0.98–1.02) | 1 (0.96–1.04) | 0.98 (0.94–1.03) | 0.96 (0.92–0.99) | 0.92 (0.89–0.96) | 0.89 (0.84–0.94) | 0.86 (0.79–0.93) | 36 | 0.130 |
| Linear | 5 (3) | Ref. | 0.99 (0.98–0.99) | 0.97 (0.96–0.99) | 0.96 (0.94–0.98) | 0.95 (0.92–0.97) | 0.93 (0.9–0.97) | 0.92 (0.88–0.96) | 0.91 (0.86–0.95) | 1% | 0.398 |
| Follow up >10 years | |||||||||||
| Non-linear | 6 (4) | Ref. | 1.02 (0.99–1.04) | 1.03 (0.98–1.09) | 1.02 (0.96–1.10) | 0.99 (0.91–1.08) | 0.95 (0.85–1.05) | 0.91 (0.79–1.03) | 0.87 (0.74–1.01) | 57% | 0.01 |
| Linear | 6 (4) | Ref. | 0.99 (0.98–1.00) | 0.97 (0.96–0.99) | 0.96 (0.93–0.99) | 0.95 (0.91–0.99) | 0.94 (0.89–0.98) | 0.93 (0.87–0.98) | 0.91 (0.85–0.98) | 21% | 0.277 |
| Follow up <10 years | |||||||||||
| Non-linear | 4 (2) | Ref. | 0.97 (0.91–1.04) | 0.95 (0.85–1.07) | 0.94 (0.83–1.07) | 0.94 (0.83–1.07) | 0.95 (0.83–1.08) | 0.95 (0.82–1.1) | 0.95 (0.80–1.12) | 43% | 0.101 |
| Linear | 4 (2) | Ref. | 0.99 (0.97–1.01) | 0.98 (0.94–1.02) | 0.97 (0.92–1.04) | 0.97 (0.89–1.05) | 0.96 (0.86–1.06) | 0.95 (0.84–1.07) | 0.94 (0.82–1.09) | 31% | 0.225 |
| No. of Datasets (No. of Studies) | Intercept (95% CI) | Slope per 1 Cup/Day (95% CI) | p for Slope | |
|---|---|---|---|---|
| SBP (mmHg) | 5 (4) | 122.3 (115.2, 129.3) | 0.01 (−0.12, 0.13) | 0.9345 |
| DBP (mmHg) | 5 (4) | 75.6 (71.2, 79.8) | −0.01 (−0.14, 0.12) | 0.9131 |
| Smokers (%) | 5 (4) | 16.9 (7.2, 26.7) | 6.49 (3.77, 9.22) | <0.001 |
| BMI | 5 (4) | 25.4 (24.1, 26.6) | 0.02 (−0.08, 0.13) | 0.6461 |
| Age (year) | 5 (4) | 48.9 (35.9, 61.8) | −0.13 (−0.42, 0.15) | 0.3565 |
| Sodium (mg/day) | 3 (2) | 2903.2 (2480.9, 3325.6) | 69.2 (37.0, 101.4) | <0.001 |
| Potassium (mg/day) | 3 (2) | 3326.6 (2613.5, 4039.7) | 38.0 (3.2, 72.8) | 0.0326 |
| Low PA (%) | 3 (2) | 26.6 (23.8, 29.4) | 0.38 (−0.83, 1.59) | 0.5391 |
| Diabetic (%) | 3 (2) | 4.48 (0.51, 8.45) | −0.81 (−1.84, 0.22) | 0.1218 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grosso, G.; Micek, A.; Godos, J.; Pajak, A.; Sciacca, S.; Bes-Rastrollo, M.; Galvano, F.; Martinez-Gonzalez, M.A. Long-Term Coffee Consumption Is Associated with Decreased Incidence of New-Onset Hypertension: A Dose–Response Meta-Analysis. Nutrients 2017, 9, 890. https://doi.org/10.3390/nu9080890
Grosso G, Micek A, Godos J, Pajak A, Sciacca S, Bes-Rastrollo M, Galvano F, Martinez-Gonzalez MA. Long-Term Coffee Consumption Is Associated with Decreased Incidence of New-Onset Hypertension: A Dose–Response Meta-Analysis. Nutrients. 2017; 9(8):890. https://doi.org/10.3390/nu9080890
Chicago/Turabian StyleGrosso, Giuseppe, Agnieszka Micek, Justyna Godos, Andrzej Pajak, Salvatore Sciacca, Maira Bes-Rastrollo, Fabio Galvano, and Miguel A. Martinez-Gonzalez. 2017. "Long-Term Coffee Consumption Is Associated with Decreased Incidence of New-Onset Hypertension: A Dose–Response Meta-Analysis" Nutrients 9, no. 8: 890. https://doi.org/10.3390/nu9080890